To schedule a consultation with Dr. Most, please call (650) 736-3223.
Serving patients from Palo Alto, San Francisco, San Jose, and throughout the Bay Area.
Crooked Nose
Approaches to Nasal Deviation & Asymmetry
This page summarizes surgical concepts for trainees and colleagues; it is not intended as medical advice.
Facial symmetry is an ideal rather than a universal reality—mild asymmetries are both natural and expected. In nasal surgery, the goal is improvement in alignment, contour, and function, not absolute symmetry. Success depends on understanding the nasal thirds: upper (bony), middle (cartilaginous), and lower (tip and base).
Evaluation and Classification
A comprehensive analysis of nasal deviation begins with facial landmarks, as shown in the frontal and basal views below.
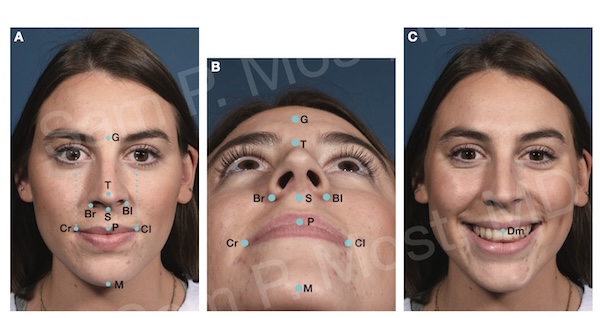
Figure 14-1: Key facial and nasal landmarks used in symmetry analysis.
The crooked nose can be categorized by location of deviation: upper third, middle third, or lower third.
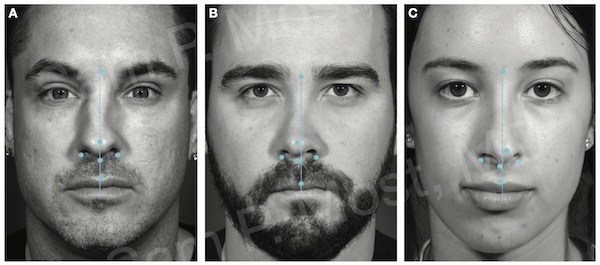
Figure 14-3: Examples of upper, middle, and lower third nasal deviations.
Correction of Upper Third Deviations
One patient with deviation isolated to the bony vault was treated using sequential open-book osteotomies. Anterior septal reconstruction (ASR) stabilized the tripod base, and a titanium plate secured the graft to the premaxilla. Tongue-in-groove (TIG) and alar-spanning sutures were used for tip support, with morselized cartilage added at the supratip.
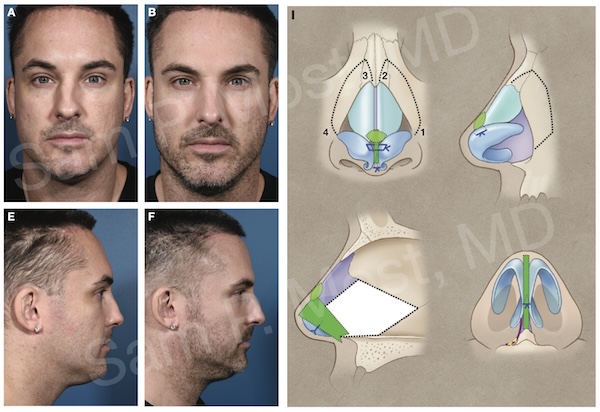
Figure 14-4: Upper third deviation treated with osteotomies and ASR.
Another patient with deviation of the upper two thirds was treated with the same osteotomy approach along with left-sided spreader and autospreader grafts. ASR was used to center the tripod base and support airway function.
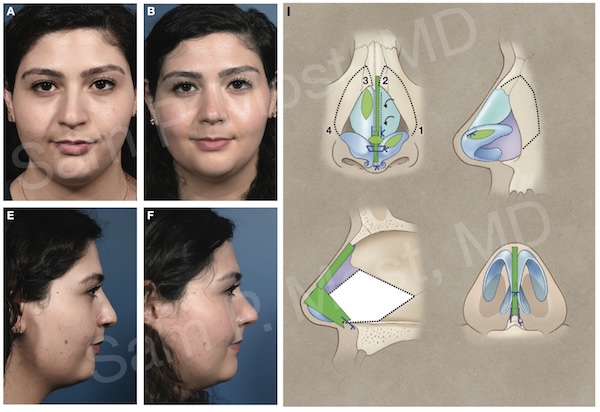
Figure 14-6: Correction of deviation with osteotomies and grafting.
Combined Upper and Middle Third Deviation
In this case, a unilateral medial osteotomy was combined with a spreader graft placed between nasal bone and septum, extending into the midvault. Morselized cartilage augmented the supratip and midvault. ASR set the base, and TIG and alar-spanning sutures aligned the tip.
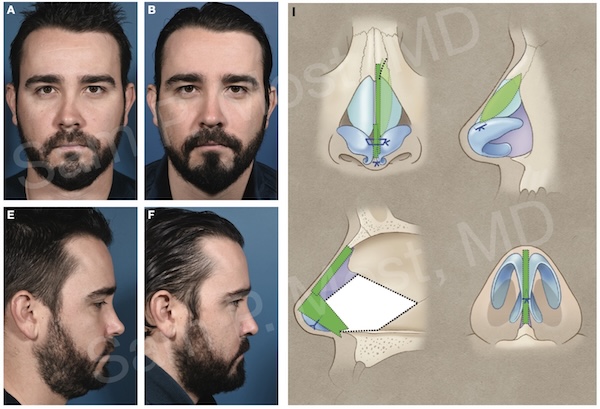
Figure 14-11: Unilateral osteotomy with dorsal and midvault augmentation.
A second patient with a wide dorsum, dorsal hump, midvault asymmetry, and tip ptosis underwent piezo-assisted hump reduction, a left-sided spreader graft, ASR, cephalic trims, mini strut grafts, and morselized cartilage over the ala.
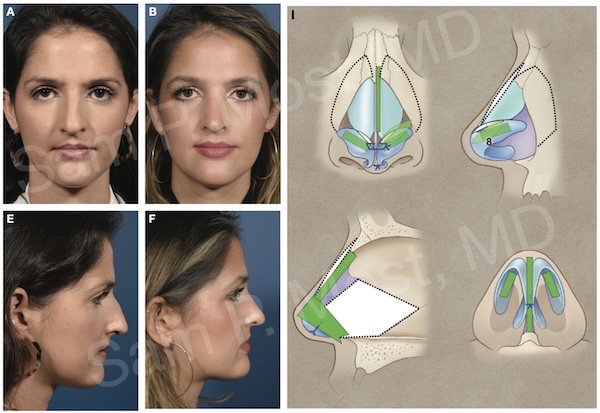
Figure 14-13: Complex deviation with dorsal work and tip support.
In a third case, post-traumatic deviation of the upper and middle thirds was corrected using piezo osteotomies, a right-sided extended spreader graft, diced rib graft with fibrin glue, and free cartilage for camouflage. Symmetry was improved by 4 months.
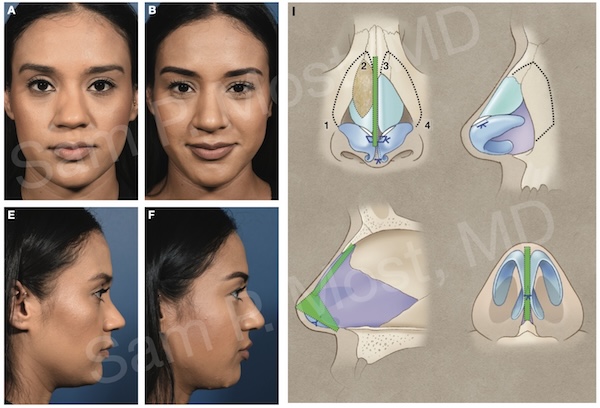
Figure 14-14: Correction of traumatic upper/midvault deviation.
Lower Third and Tip Deviation
Tip deviation following prior rhinoplasty was managed using ASR with miniplate fixation, a clocking suture, and a mini strut graft. Morselized cartilage was placed under thin skin for camouflage.
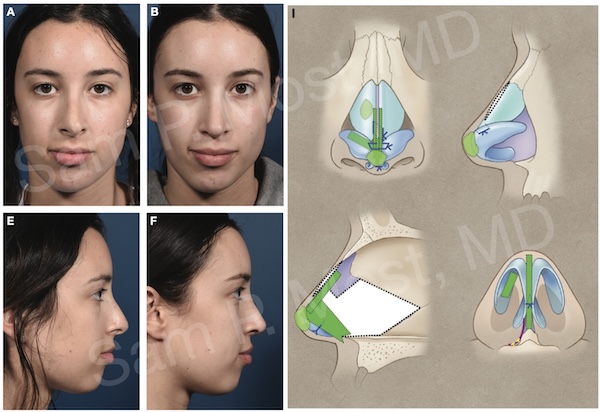
Figure 14-15: Correction of lower third deviation after prior surgery.
Another patient with deviation of the lower two thirds, a dorsal hump, and airway compromise underwent Joseph hump reduction, ASR with miniplate, bilateral autospreader grafts, and a left-sided spreader graft.
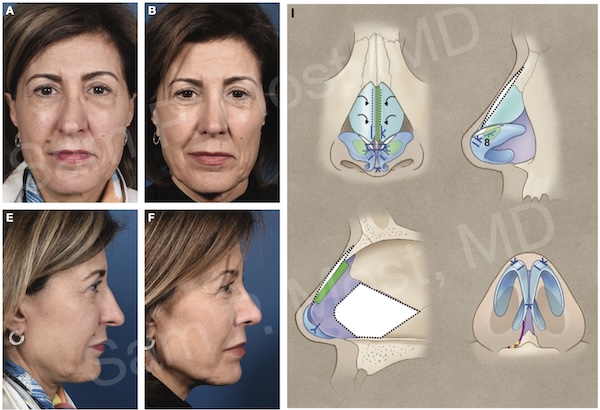
Figure 14-16: Combined deviation and airway treatment.
Dorsal Preservation for Crooked Noses
Using the Modified Subdorsal Strip Method (MSSM), the osseocartilaginous vault can be mobilized laterally and fixed to the dorsal remnant. This technique allows correction of deviation in the upper and middle thirds while preserving dorsal lines.
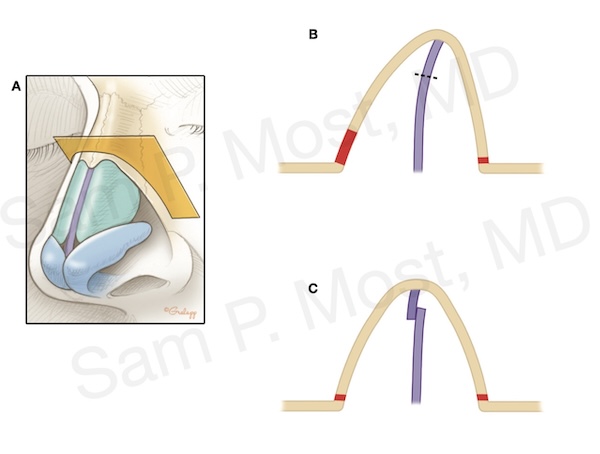
Figure 14-18: MSSM used to correct dorsal asymmetry via preservation method.
Summary
While complete nasal symmetry is neither achievable nor expected, structured and individualized treatment approaches—ranging from osteotomies and spreader grafts to ASR and preservation techniques—can restore balance and function. The crooked nose requires nuanced analysis and a multi-level surgical strategy to achieve natural, harmonious results.